Lee Jk Restoration of Primary Anterior Teeth Review of the Literature
An exploration of esthetic crown options for deciduous teeth, and the evidence supporting their use
In modern society, the demand for esthetic restorations is increasing in pediatric dentistry. Parents have high expectations of the restorative materials, especially in the esthetic zone. Durability, toll and esthetics are the primary factors considered by parents when determining a treatment plan.1 Molar-colored restorations, especially for anterior teeth, are of chief concern to parents. A particular study showed that parents ranked attractiveness and health similarly.2 The same study likewise mentioned that parents viewed silvery stainless steel crowns equally unhealthy and esthetically unacceptable. While the decision on treatment planning is oft driven by the parents,three children are too concerned almost esthetics and tend to prefer white fillings rather than silver.4
Minimal research is available to provide evidence of the comparative clinical success of various esthetic crowns for primary teeth. Recommendations for esthetic total coverage crowns in the primary dentition are based on limited enquiry, mainly relying on retrospective studies and case reports. Well-controlled randomized clinical trials are difficult to implement in children due to financial, behavioral and social barriers.
This commodity will discuss the possible esthetic crown options in anterior teeth, and the bachelor testify to support the use of diverse restorations.
STAINLESS STEEL CROWNS AND OPEN-FACED STAINLESS STEEL CROWNS
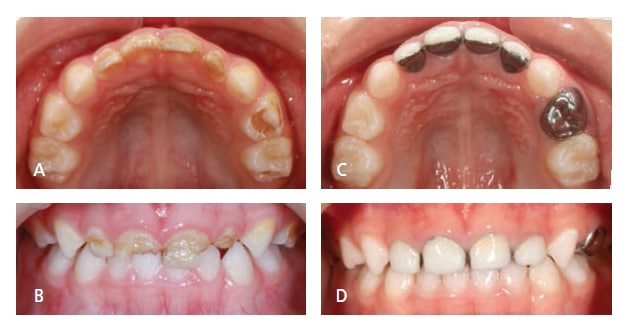
FIGURES 1A THROUGH 1D COURTESY YI-CHUN CHEN, DDS
Stainless steel crowns (SSCs) tin can restore inductive teeth with all-encompassing caries just still provide a stable restoration. This blazon of crown is resistant to fracture and can be easily fitted likewise as crimped on all surfaces, fifty-fifty when there is minimal remaining tooth nowadays.v The dissatisfying silvery color can be improved by the open-confront stainless steel crown technique.six,seven Later the recommended glass ionomer cement is gear up, the metallic on the facial surface of the crown is removed by a 330 bur. Tooth-colored resin is placed later on etching and bonding (Figures 1A through 1D). This open-face technique is cheap and can provide a better esthetic advent compared to the original silvery metal color — however, it is time consuming, and esthetics are compromised past the metal margin. Hemorrhage control is extremely of import when placing the resin, and it is often difficult to control bleeding after the SSC tooth preparation. SSCs are less frequently used in primary inductive teeth than posterior teeth, merely due to the occlusion or extensive caries, they are sometimes used in anterior teeth. SSCs are more commonly applied to the mandibular incisors, where esthetics is less noticeable. The memory charge per unit of SSCs is reported as 93% subsequently 27 months and SSCs appear to exist retained significantly longer than preveneered SSCs.viii
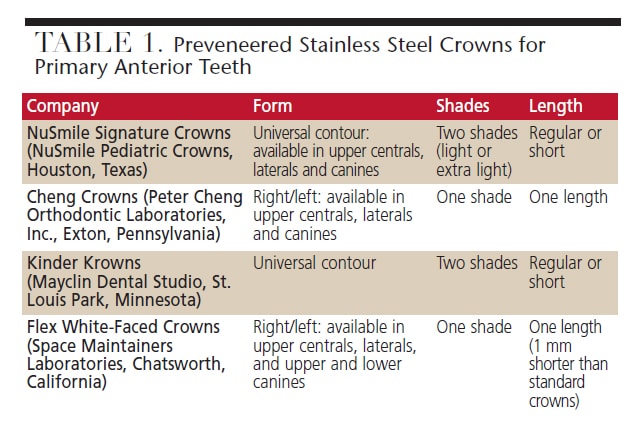
PREVENEERED STAINLESS STEEL CROWNS
Preveneered SSCs were introduced into the pediatric dentistry market place to provide some other esthetic pick for anterior restorations. These crowns accept prefabricated tooth-colored cloth bonded to SSCs on the facial surface, unremarkably with resin-based composite material. Various brands are listed in Table i. The prefabricated esthetic facial surface enables the crown to be placed in an area with poor hemorrhage control, providing a white appearance (Figures 2A and 2B).9–11
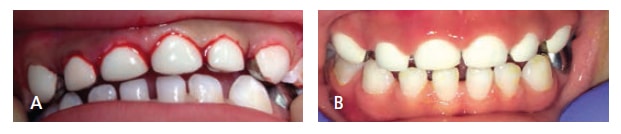
FIGURES 2A AND 2B COURTESY JEROD BRAZEAL, DDS
The chief trouble with these crowns is the possible wearable on the incisal border, equally well every bit partial or total fracture of the facial portion. It is hard to repair the chipped portion and if parents or children are concerned about a portion of metal showing, the replacement of the whole crown is needed. Several studies have shown that 12% to 39% of preveneered crowns have wear or partial facing loss.9–xi Total loss of the esthetic facing was reported to range up to 24% of the preveneered crowns in these studies.
Crimping of the facial preveneered portion will crusade esthetic facing to fracture easily. Thus, retention of the crowns relies on crimping the lingual portion of the crown. When applying the crown, it must not be forced over the prepared tooth considering the prefabricated resin portion is easily fractured. When cementing these crowns, it is recommended to use glass ionomer cement to hold the crown in place until the cement sets. The retention rate for this blazon of crown is reported to exist above 90% subsequently half dozen to 17 months.8–11
A contempo prospective study compared parental satisfaction of three different molar-colored inductive crowns.12 The study showed that parents are least satisfied with preveneered SSCs when compared with zirconia and strip crowns, mainly due to the color. In some other study by Champagne et al,13 however, the parental satisfaction was 93% at 13 months mail service crown placement. Fifty-fifty though the lingual portion of the crown was argent, parents had high satisfaction with these crowns.
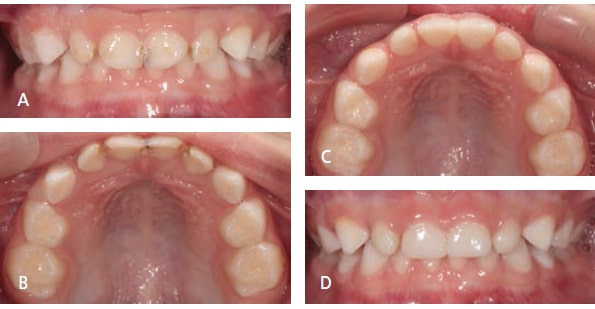
STRIP CROWNS
This blazon of crown is composed of celluloid crown forms that act as matrix forms to fill with tooth-colored materials. Usually, these crowns are restored with resin-based blended to permit for selection of shades to match the adjacent teeth and provide an splendid esthetic event (Figures 3A through 3D). Resin modified glass ionomer cement has been used for the material as an acting restoration in younger children.14,fifteen Placing a strip crown is technique-sensitive considering wet and hemorrhage control are very important to prevent contagion of the resin with blood or saliva. There must exist enough remaining tooth structure to let for adequate bonding.5 Afterwards the polymerization of the resin-based composite, the celluloid class tin exist hands removed with a dental bur or a sharp bract.
When placing strip crowns over pulpectomy treated teeth obturated with iodoform paste, information technology is important to utilise opaque resin or remove iodoform paste below the cervical area then the yellow iodoform paste will non be seen through the strip crown from the facial surface (Figures 4A and 4B).16 Besides, teeth that take been restored with zinc-oxide eugenol after pulpal treatment should have a glass ionomer or resin modified glass ionomer base placed over the zinc-oxide eugenol then that polymerization upon calorie-free exposure is non compromised. Overall, parental satisfaction was excellent for this type of crown. I study showed that parents preferred strip crowns to preveneered crowns.12 However, fractional or full loss of the crown or durability was the principal concerns from parents.12,17 Studies show that the overall retention rate was higher up 80% later xviii to 24 months.16,18

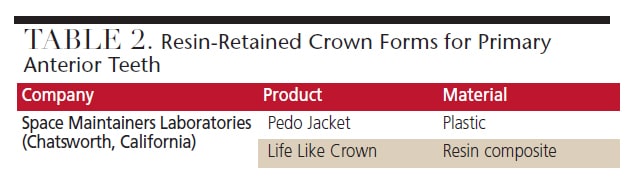
RESIN-RETAINED CROWN FORMS
Besides the widely used strip crowns, at that place are 2 alternatives that bind to the tooth structure (Tabular array two). One is made of a tooth-colored plastic. Afterward the molar is etched and bonded, a crown filled with resin material is fitted to the tooth. There is no demand to remove the crown form after polymerization. However, the crown cannot be reshaped with a bur because the plastic material volition disform from the oestrus. The other culling is made of resin composite cloth and tin can be reshaped with a finishing bur to provide a more esthetically pleasing appearance. If the tooth is not reduced adequately, forcing the crown down to the molar can crusade the crown to crack or fracture.
ZIRCONIA CROWNS

FIGURE 5 COURTESY MARIA JOSE CERVANTES MENDEZ, DDS, MS
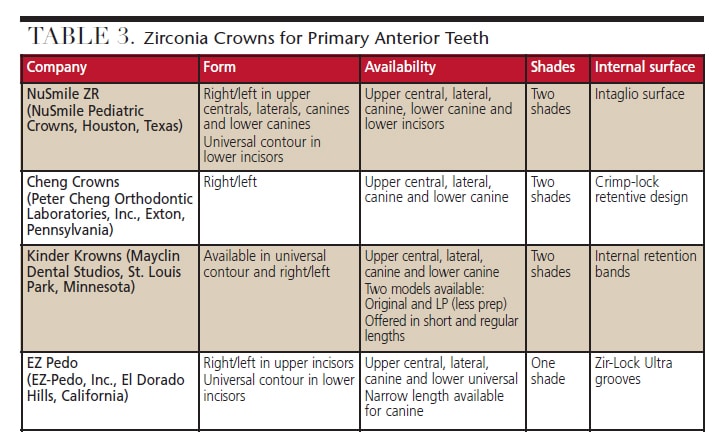
Zirconia crowns have been successfully used for permanent teeth for many years and provide excellent esthetics due to their natural appearance. Zirconia crowns are relatively new in the practice of pediatric dentistry, introduced in 2010. They are recommended for both anterior and posterior cases. Table 3 lists the products bachelor in this category for the primary inductive dentition. Zirconia crowns are very strong, durable and esthetically pleasing (Effigy 5). Unfortunately, since these preformed crowns cannot be crimped, the memory is reliant on the internal surface designs (Table 3) and cementation.
In that location is a learning curve for dentists who are unfamiliar with placing pediatric zirconia restorations. Information technology may take longer to set up the tooth and fit the crown because the tooth is prepared to fit the crowns rather than only adjusting crowns to fit a molar. Zirconia crowns crave a feathered margin as in other crown preparations; all the same, these crowns demand more than tooth reduction when compared to strip crowns and SSCs. One written report showed that there is no significant departure in tooth reduction for inductive zirconia crowns between the four brands available.19
Hemorrhage control is of import to prevent contamination of the crowns and reach acceptable bonding.20 Generally, these crowns require thorough cleaning with alcohol before final cementation, although one brand includes try-in crowns for trial fitting, which allows the final crown to remain contamination-free prior to cementation. About manufacturers recommend glass ionomer cement or resin modified glass ionomer to cement zirconia crowns — however a bioactive resin cement has as well been recommended by a manufacturer.
In that location are very few studies evaluating the clinical use of zirconia crowns in primary inductive and posterior teeth.12,21–24 Ane randomized controlled trial with a short follow-upward period of six months was conducted.22 In this study, 129 teeth were randomly distributed into one of the three handling groups (strip crowns, preveneered SSCs or zirconia crowns). Zirconia crowns showed the highest retention rate (100%) and better gingival health adaptation, whereas preveneered SSCs had a 95% retention rate and strip crowns had a retentivity rate of 78%.
A retrospective report was performed to examine 44 anterior crowns for an boilerplate of 20.viii months after placement.21 There was no wear observed on any teeth opposing the crowns. Among the parents/caregivers in the written report, 78% reported that the crowns improved appearance. The overall satisfaction from parents/caregivers with these crowns was very high (ix.iii out of possible 10).
A prospective written report to compare parental satisfaction was conducted using three dissimilar molar-colored anterior crowns.12 This study showed that parents had the highest satisfaction with zirconia crowns, followed past strip crowns and preveneered SSCs.
KEY TAKEAWAYS
- Stainless steel crowns are a stable restoration selection for inductive teeth with extensive caries. The open-face up technique tin provide a ameliorate esthetic advent compared to the original silver metal color.
- A prefabricated esthetic facial surface enables preveneered stainless steel crowns to exist placed in an expanse with poor hemorrhage control, providing a white appearance. The main trouble is the possible fracture of the facial portion, which is difficult to repair.
- Strip crowns are used in cases with plenty remaining molar construction to allow for adequate bonding. Placing strip crowns is technique-sensitive because moisture and hemorrhage control are important to preclude contamination of the resin with claret or saliva.
- Zirconia crowns are relatively new in pediatric dentistry and require a learning curve for dentists. These crowns cannot be crimped, and hemorrhage control is important to prevent contagion of the crowns and achieve adequate bonding.
CONCLUSION
Clinically, the choice of the crown depends on the preference of the operator, behavior of the patient, occlusion, amount of remaining tooth construction, and parental expectations. There has withal to be a clinical study to show which restoration is considered the best. Further well-controlled randomized clinical trials are needed to enable clinicians to brand the best evidence-based decisions.
REFERENCES
- Tinanoff N, Douglass JM. Clinical decision-making for caries management in primary teeth. J Paring Educ. 2001;65:1133–1142.
- Woo D, Sheller B, Williams B, Mancl 50, Grembowski D. Dentists' and parents' perceptions of health, esthetics, and treatment of maxillary primary incisors. Pediatr Dent. 2005;27:nineteen–23.
- Zimmerman JA, Feigal RJ, Till MJ, Hodges JS. Parental attitudes on restorative materials as factors influencing current utilize in pediatric dentistry. Pediatr Dent. 2009;31:63–lxx.
- Fishman R, Guelmann M, Bimstein E. Children's option of posterior restorative materials. J Clin Pediatr Dent. 2006;31:1–4.
- Waggoner WF. Restorative dentistry for the principal dentition. In: Casamassimo PS, Fields H, McTigue D, Nowak A, eds. Pediatric Dentistry: Infancy Through Adolescence. fifth ed. Phiadelphia, Penn: WB Saunders Co/ Elsevier Inc; 2013:304–332.
- Hartmann CR. The open-face stainless steel crown: an esthetic technique. ASDC J Dent Child. 1983;fifty:31–33.
- Helpin ML. The open up-face up steel crown restoration in children. ASDC J Dent Child. 1983;50:34–38.
- Lopez-Loverich AM, Garcia MM, Donly KJ. Retrospective study of retention of stainless steel crowns and pre-veneered crowns on master anterior teeth. Pediatr Dent. 2015;37:530–534.
- Roberts C, Lee JY, Wright JT. Clinical evaluation of and parental satisfaction with resin-faced stainless steel crowns. Pediatr Paring. 2001;23:28–31.
- Shah PV, Lee JY, Wright JT. Clinical success and parental satisfaction with anterior preveneered chief stainless steel crowns. Pediatr Dent. 2004;26:391–395.
- MacLean JK, Champagne CE, Waggoner WF, Ditmyer MM, Casamassimo P. Clinical outcomes for master anterior teeth treated with preveneered stainless steel crowns. Pediatr Dent. 2007;29:377–381.
- Salami A, Walia T, Bashiri R. Comparison of parental satisfaction with three tooth-colored full-coronal restorations in chief maxillary incisors. J Clin Pediatr Dent. 2015;39:423–428.
- Champagne C, Waggoner West, Ditmyer One thousand, Casamassimo PS, MacLean J. Parental satisfaction with preveneered stainless steel crowns for primary anterior teeth. Pediatr Dent. 2007;29:465–469.
- Jeong MA, Kim AH, Shim YS, An SY. Restoration of strip crown with a resin-bonded composite cement in early childhood caries. Example Rep Dent. 2013;2013:581934.
- Nelson T. An improved acting therapeutic restoration technique for management of anterior early childhood caries: report of ii cases. Pediatr Paring. 2013;35:124–128.
- Kupietzky A, Waggoner WF, Galea J. The clinical and radiographic success of bonded resin composite strip crowns for primary incisors. Pediatr Dent. 2003;25:577–581.
- Kupietzky A, Waggoner WF. Parental satisfaction with bonded resin blended strip crowns for master incisors. Pediatr Dent. 2004;26:337–340.
- Ram D, Fuks AB. Clinical performance of resin-bonded composite strip crowns in primary incisors: a retrospective study. Int J Paediatr Dent. 2006;16:49–54.
- Clark Fifty, Wells MH, Harris EF, Lou J. Comparison of amount of primary tooth reduction required for anterior and posterior zirconia and stainless steel crowns. Pediatr Dent. 2016;38:42–46.
- Waggoner WF. Restoring chief anterior teeth: updated for 2014. Pediatr Dent. 2015;37:163–170.
- Holsinger DM, Wells MH, Scarbecz M, Donaldson Thousand. Clinical evaluation and parental satisfaction with pediatric zirconia inductive crowns. Pediatr Paring. 2016;38:192–197.
- Walia T, Salami AA, Bashiri R, Hamoodi OM, Rashid F. A randomised controlled trial of three aesthetic full-coronal restorations in principal maxillary teeth. Eur J Paediatr Dent. 2014;15:113–118.
- Ashima G, Sarabjot KB, Gauba Thousand, Mittal HC. Zirconia crowns for rehabilitation of decayed main incisors: an esthetic alternative. J Clin Pediatr Dent. 2014;39:18–22.
- Planells del Pozo P, Fuks AB. Zirconia crowns — an esthetic and resistant restorative culling for ECC affected primary teeth. J Clin Pediatr Paring. 2014;38:193–195.
FEATURED Photograph COURTESY OF LUCKYBUSINESS/ISTOCK/ THINKSTOCK
From Decisions in Dentistry . October 2016;2(ten):18, 21-25.
Source: https://decisionsindentistry.com/article/review-esthetic-crowns-primary-anterior-dentition/
0 Response to "Lee Jk Restoration of Primary Anterior Teeth Review of the Literature"
Post a Comment